This week, I attended a Becker’s ASC Review webinar on why sterile processing failures in ASCs are a bottom-line problem, with Damien Berg and Jeremy Gibson-Roark RN, BSN, MBA, CIC, CNOR. I went as the co-founder of a company that builds instrument tracking technology. I left more convinced than ever that they were right about something that, on its face, argues against my own business.
At one point they told the audience: you don’t need to go buy an instrument tracking system. They also made the case that most published standards are written around big-box hospitals, not ambulatory surgery centers.
I agree with both statements. And I want to explain with nuance why those statements have been shifting my outlook on what ASCs actually need, and why “buy a tracking system” was the wrong prescription long before anyone said so out loud.
The work outgrew the tools
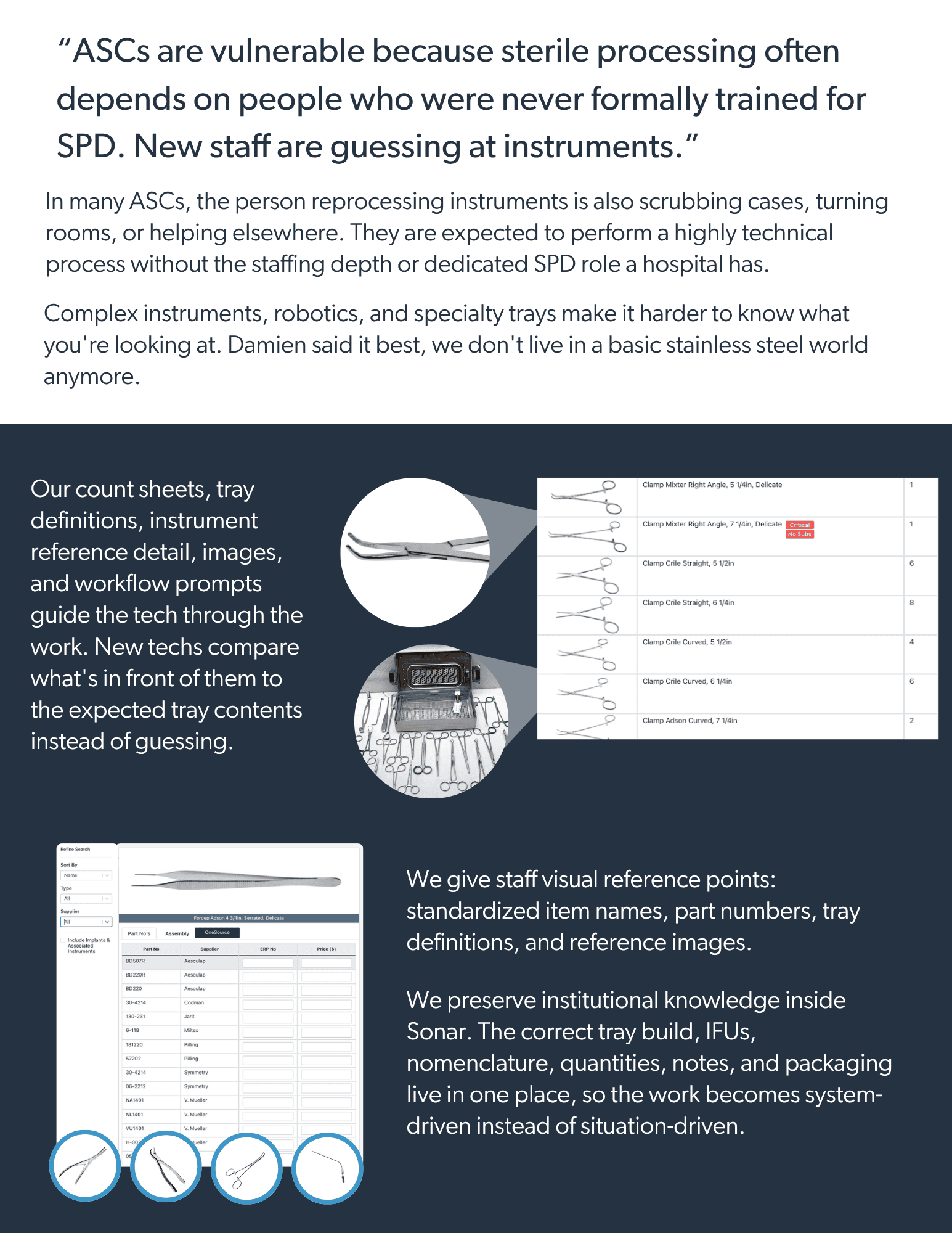
Surgical care has moved out of the hospital. More than 80% of U.S. surgeries now happen in outpatient settings, and ASC procedure volumes are forecast to grow 21% over the next decade. The cases are harder too. Robotics, complex instrument sets, tighter turnovers. As Berg put it, we don’t live in a basic stainless steel world anymore.
So you have rising volume and rising complexity landing on departments that run lean. In a lot of ASCs, the same person scrubs in during the day and reprocesses instruments at the end of it, often without dedicated sterile processing training. That is not a knock on the people. It is a description of the pressure.
Where it breaks, quietly
Berg and Gibson-Roark were specific about where systems break down, and none of it was dramatic. The failures are ordinary, and they compound.
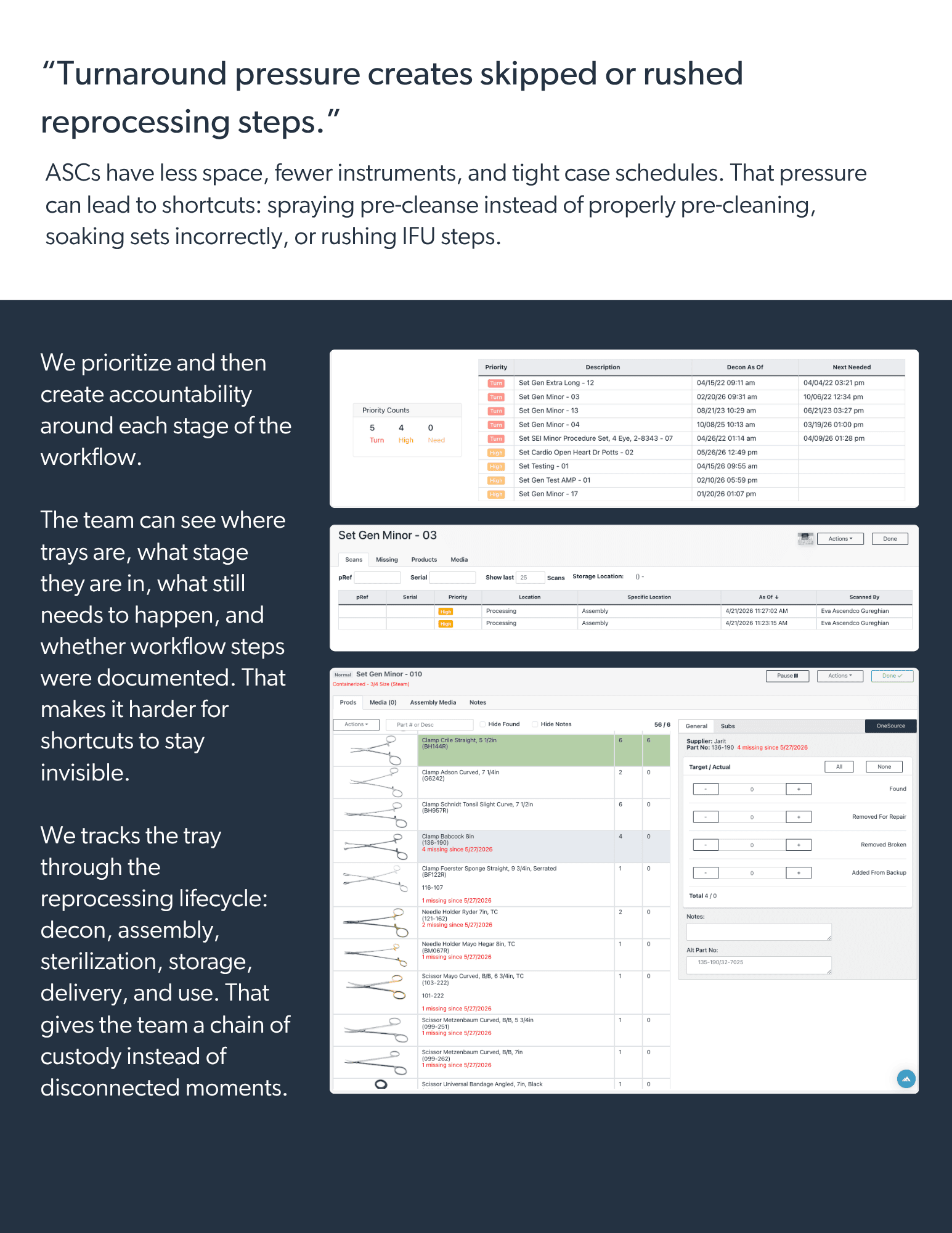
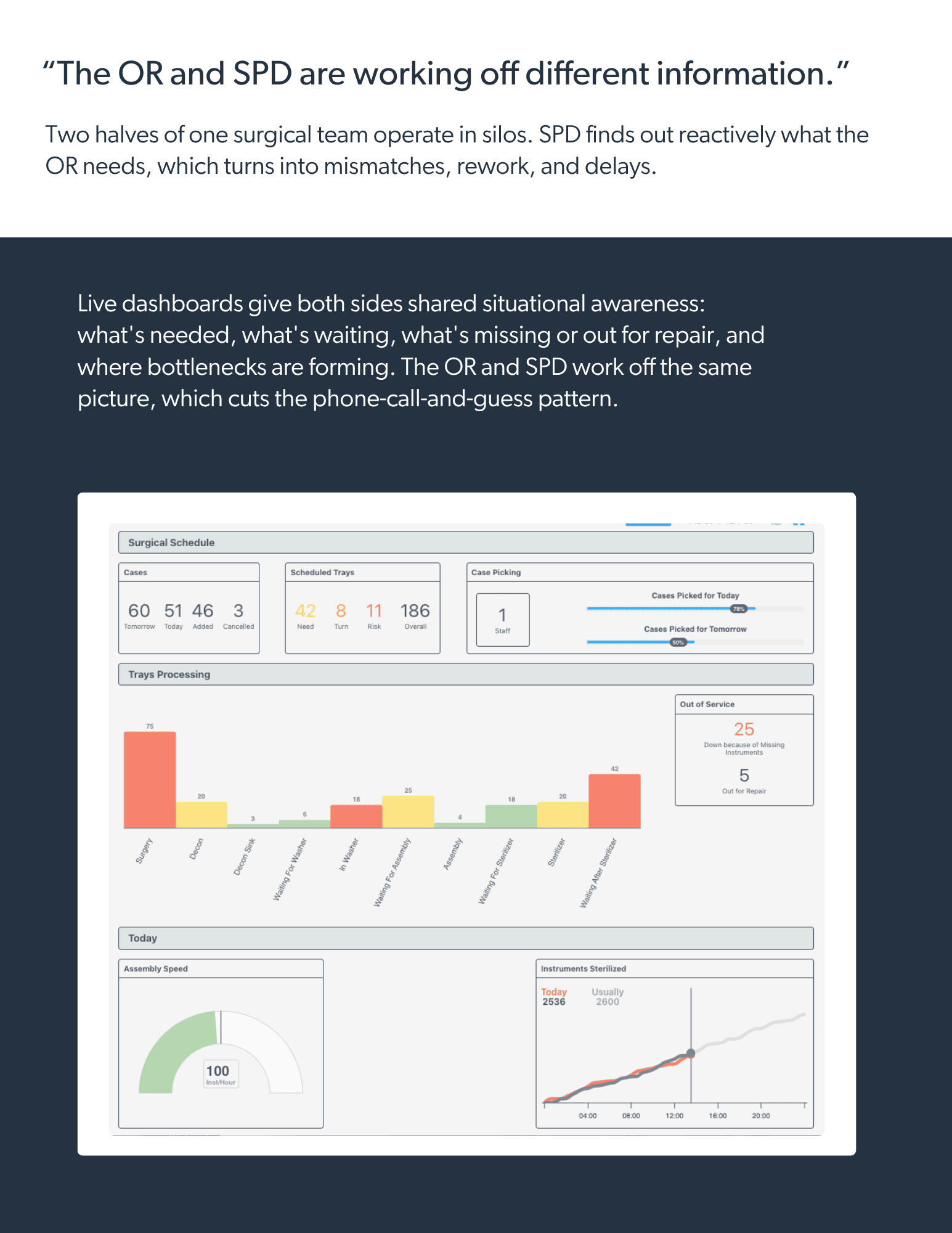
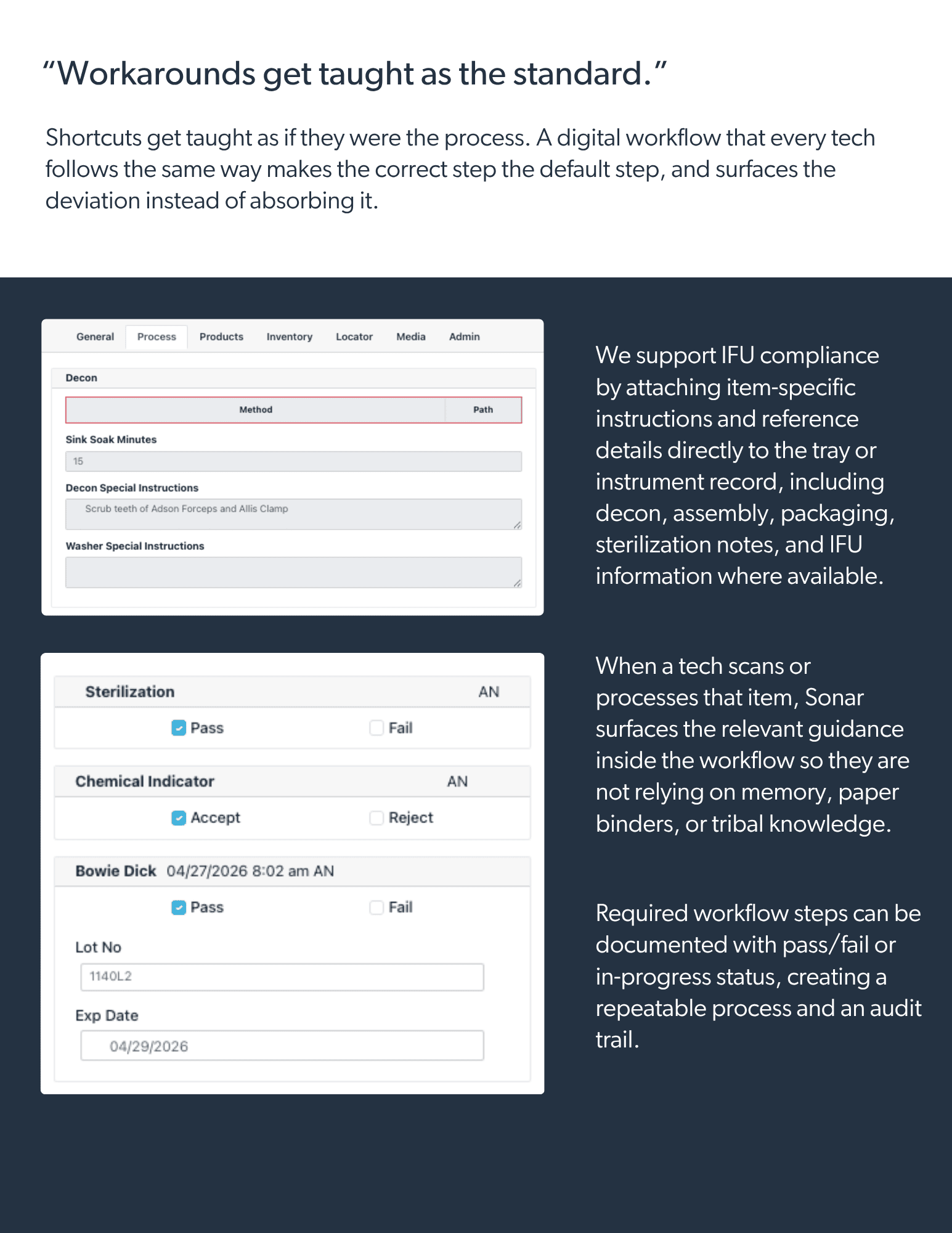
Departments run on cultural and tribal knowledge, and they implement workarounds because that’s how they were trained, not because anyone documented the right way. There’s a staffing vulnerability rooted in a lack of training, knowledge, and competency, with techs wearing multiple hats. Turnaround pressure compresses the steps, so corners get cut: spraying a pre-cleanse instead of actually pre-cleaning, or letting sets sit overnight in enzymatic detergent that has long since stopped doing its job. The OR and SPD operate in silos, with miscommunication that turns into rework and delay. And underneath all of it sit the risks that stay invisible until they’re not: biofilm, water quality, traceability gaps, documentation gaps.
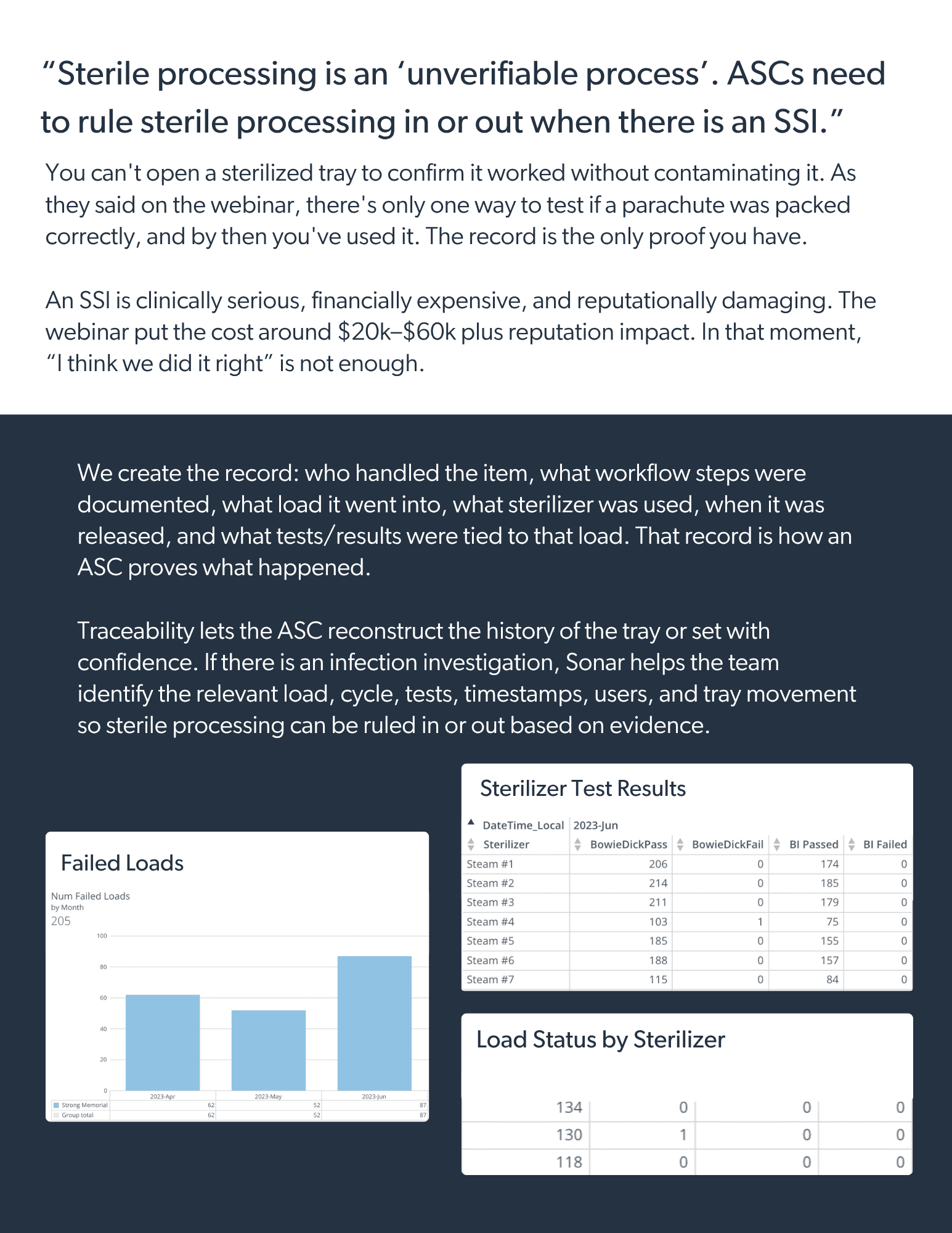
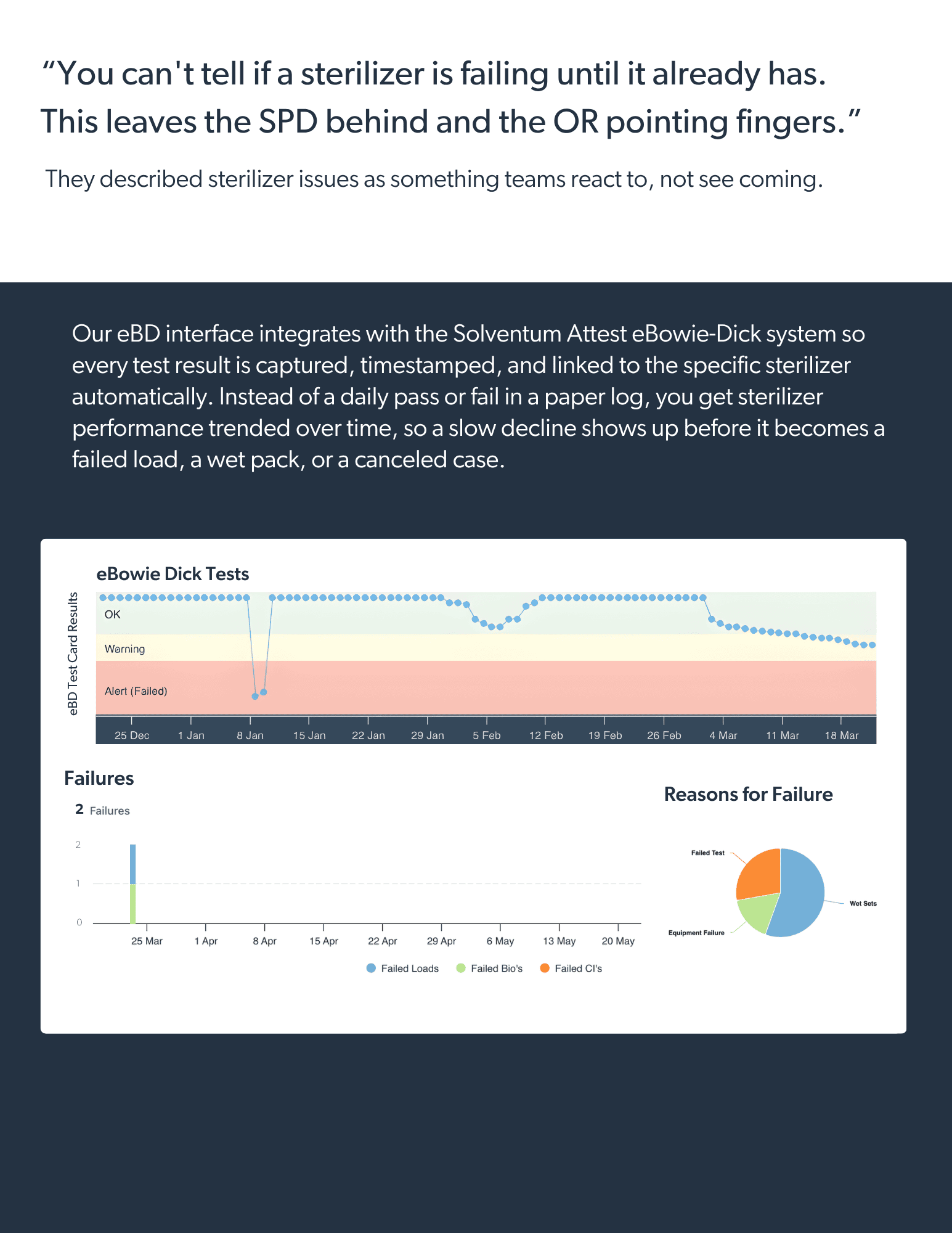
The sharpest point was their description of sterile processing as an unverifiable process. You cannot open a sterilized tray to confirm it worked without contaminating it. The only protection is the record. And in the event of a surgical site infection, the only way to rule sterile processing in or out as the cause is a complete, traceable trail back to that specific tray.
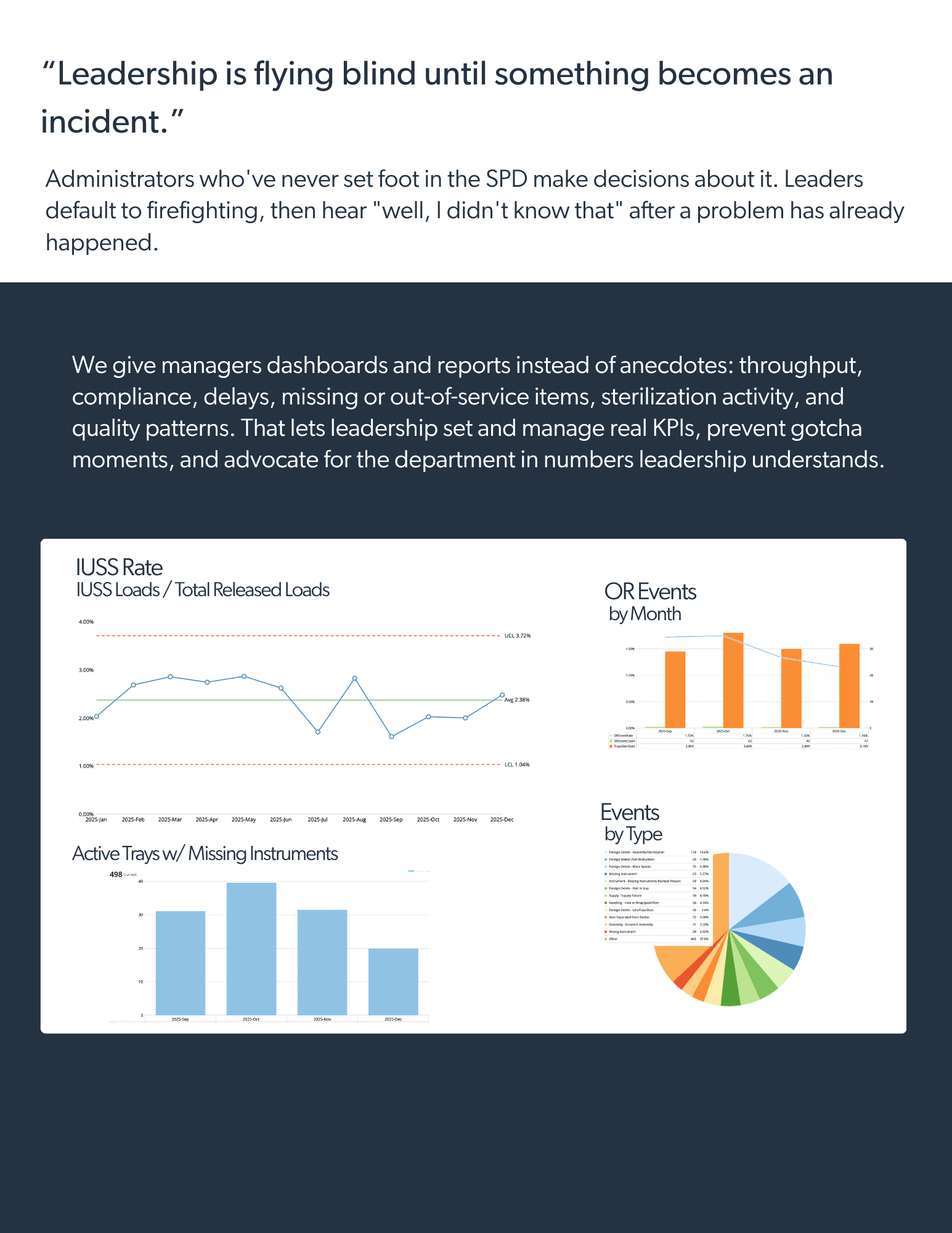
They also named the leadership problem honestly. Administrators who have never set foot in the SPD making decisions about it. Leaders defaulting to day-to-day firefighting with their head in the sand, then learning about a problem only after it becomes an incident. Their suggestion was the right one: get visible, and set KPIs that prevent gotcha moments instead of reacting to them.
Why “don’t buy a tracking system” was right
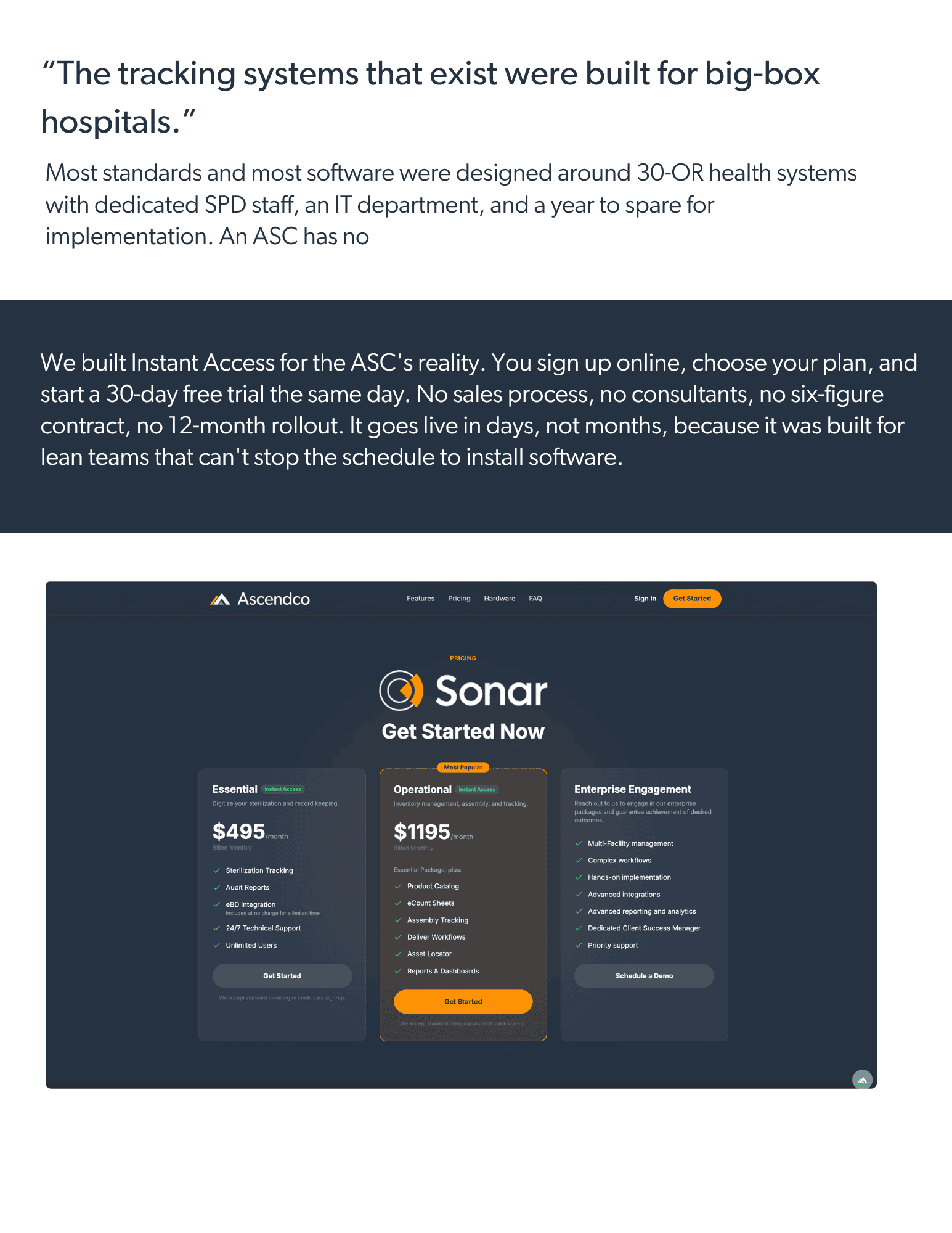
Here is the part I want every ASC leader to hear clearly. When the experts say don’t buy a tracking system, they are right, because the systems on the market were built for big-box hospitals.
Think about what that actually means in practice. A 30-OR academic medical center has a dedicated SPD with specialized staff, an IT department, a capital budget, and the bandwidth to run a 12-month implementation with onsite consultants. The tracking systems were designed around that reality: heavy configuration, long rollouts, six-figure contracts, and training programs that assume full-time sterile processing professionals on the receiving end.
Now hand that to a four-OR surgery center where the scrub tech is also the reprocessing tech, there’s no IT lift to spare, and nobody has a year to wait. It doesn’t fit. The implementation alone is a non-starter. So the ASC does the rational thing: it declines the enterprise system and goes back to paper count sheets and clipboards. And the workarounds continue, not because the team doesn’t care, but because the only tool offered was built for someone else.
That mismatch is the real problem. It was never that ASCs don’t need tracking. It’s that the tracking that existed was never shaped for them.
So we built it for you instead
I’ve spent years with a front-row seat to the workarounds facilities create. I’ve watched lean teams normalize risk because the alternative felt impossible with the resources they had. So we built the thing the market was missing: Instant Access, instrument tracking designed from the ground up for how an ASC actually operates.
When we say “Instant Access,” we mean: we can get your team live today. Without hardware installs, long IT projects, or waiting months to start standardizing. You sign up, we configure your site, and you can start building consistency immediately. For a sterile processing team, that matters because most of the risk you listed comes from one thing: work has to be done the same way, by every person, on every shift, even when staffing is thin and time is tight. Instant Access is how we make that realistic.
Once it’s live, it answers the exact problems Berg and Gibson-Roark named: staffing vulnerability, increased volume and complexity, the disconnect between departments, normalized corner cutting, leadership who doesn’t understand SPD. Let me take their list and show, plainly, what changes.
The only question that matters
The most important point they made all session was not about technology at all. They asked the room to think about who the customer really is. Not the surgeon. Not the schedule. The patient on the table, who is somebody’s mother, somebody’s son, somebody’s daughter. They asked everyone to picture their own family member there, and to think about how they would want that person’s instruments handled.
Sit with that question honestly, because it reframes everything else. The standard is simple: ASCs deserve the same level of traceability and quality oversight that health systems expect from acute care environments. Smaller footprint, leaner team, same patient. The proof her tray was processed correctly should not come down to someone’s memory of a busy shift. It should be a documented sterilization cycle, instrument detail tied to her set, and a complete record of every step from decontamination to the OR.
That is what tracking built for an ASC actually delivers. Not paperwork for its own sake, but the ability to stand behind the care. And the shift is concrete.
|
Current ASCs often look like:
|
Modern ASCs look like:
|
|---|---|
|
Paper count sheets
|
Digital decontamination instructions
|
|
Manual sterilizer logs
|
Automated cycle documentation
|
|
Verbal handoffs
|
Real-time tray location visibility
|
|
Limited visibility into missing trays
|
Procedure-level traceability
|
And the results follow. Facilities have reduced:
- IUSS utilization
- Return-to-decontamination events
- Sterile returns
- Tray search time
That is the difference between guessing and knowing, and it is achievable for an ASC without a hospital’s budget, IT department, or timeline.
So here I am, humbly making the case that ASCs do need instrument tracking. Not the big-box kind. The kind built for them and their specific problems.
My thanks to Damien Berg, Jeremy Gibson-Roark, and the Becker’s ASC Review team for a conversation worth having.
